Before we can weigh the pros and cons of the note, we need to understand what exactly a note is, and how it operates in the current documentation paradigm. The simplest answer to this seemingly odd question is that a note is a discrete bundle of related clinical information: a set of facts, opinions, and thoughts wrapped up in a single document package. The note isn’t meant to hold the entirety of a patient’s medical history or all the reasoning attached to it — it’s only a small part of the whole chart.
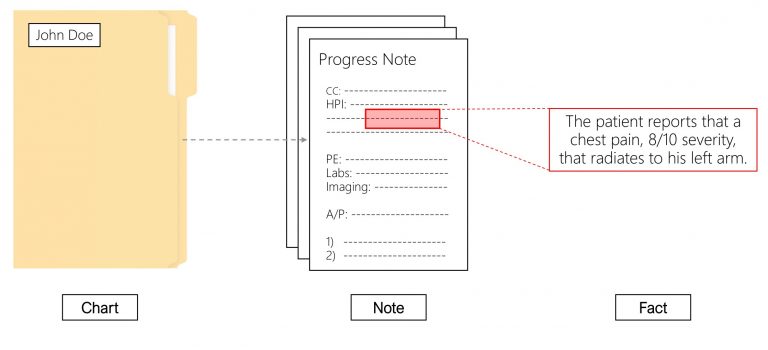
Figure 1.1. Under the current paradigm, a set of clinical facts makes up a note, and a set of notes (along with additional structured data) makes up a chart.
This three-level hierarchy — fact, note, chart — is so familiar that it has become invisible. But the middle layer is a choice, and everything in this book turns on examining that choice. Why do we bundle certain clinical facts together into “notes” at all? What work is the bundle doing? When we look closely, the note performs three distinct bundling functions at once: it groups information by time, by clinical thread, and by responsibility. Each function is legitimate. The trouble, as we will see, comes from welding all three into a single, indivisible object.
2.1 The note bundles information by time
Most fundamentally, we bundle facts into notes based on time. Each note is meant to capture a discrete timeslice of a patient’s medical life. To simplify for now (we will deal with the complexities of the multi-member medical team soon enough), think of a patient who is seen repeatedly by only one clinician. The clinician interacts with the patient at particular time points, when the patient needs medical care. In between those points, the patient is living their normal life, and the clinician is effectively in the dark. At each encounter, the clinician collects, acts on, and records all relevant information from the intervening chunk of time. That chunk varies drastically in length — from a single day (inpatient hospital rounds) to multiple years (a healthy person’s outpatient primary care visits) — but the chunks are sequential and non-overlapping.
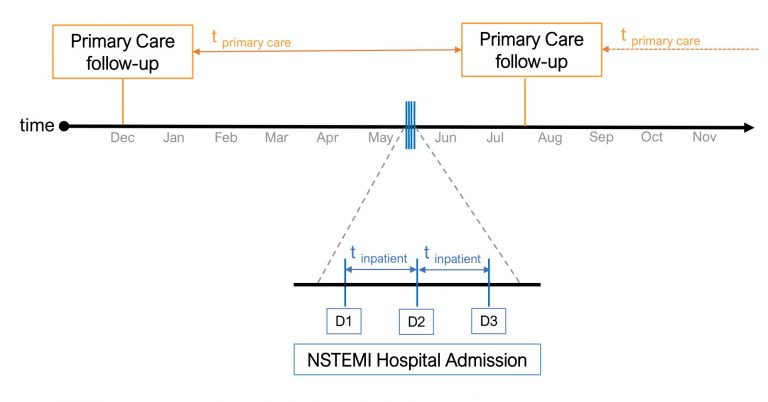
Figure 1.2. The note as timeslice. Each tick represents a note in a patient’s chart. Notes provide updates on a patient’s status over a period of time. The length of that period depends on the nature of the note: a routine primary care note updates the patient’s status after several months; during an inpatient admission, a new note updates the patient’s status each day.
The individual note, then, captures all relevant data between the last encounter and the current one — progression of illness, medication adherence, new issues — as well as what happened at the current encounter: conversations, reasoning, recommendations. Immediately after an encounter, the most recent information is reflected in the latest note, and the entire history of the patient from birth to the present is captured in the set of all existing notes — the chart. In this highly simplified model, each fact is captured exactly once, in whichever timeslice it falls into.
On the whole, non-overlapping timeslices make sense as a way to bundle facts. When searching a chart, it is easy to sort the bundles by time to find a particular event or track an evolving disease course. On the input side, documentation events map neatly onto patient encounters: most new information is acquired when a clinician sees a patient, and the clinician can document the bundle of new facts just afterward.
But the non-overlapping timeslice model isn’t perfect — some clinical information simply doesn’t fit. Most notes include summarizations of information from past timeslices (past medical history, “one-liner” summary statements, problem-level assessments), so we cannot truly say a note contains only information from its own timeslice. Newly documented events may recontextualize or change the interpretation of data recorded earlier; previously documented information may be found to be erroneous — and in these scenarios, one must read a more recent note to truly understand an older note’s timeslice. Certain information, such as cited research knowledge, doesn’t map to any timeslice at all. And clinicians routinely document the same information in multiple separate timeslices, breaking the non-overlapping ideal in practice.
For these reasons and more, a world of perfectly non-overlapping time-sliced bundles is unachievable. Nonetheless, the timeslice ideal should be a guiding principle of any sensible documentation paradigm — it is what minimizes redocumentation, minimizes the introduction of errors, and enables effective searching and sorting by time. Hold on to this: there are many possible ways to implement informational timeslices, and the modern note is only one of them.
2.2 The note bundles information by clinical thread
A second reason we bundle certain facts together — and keep others separate — relates to clinical threads. We define a thread as a stream of clinical reasoning and action that persists across multiple timeslices: the sequence of daily nursing notes during a hospital stay, a series of primary care notes over a lifetime, the sequential notes of an inpatient neurology consult. In general (though not always), clinical threads map onto the different aspects of care provided by different services. Different clinicians can be part of the same thread when they are responsible for managing the same bundle of information over time — night-shift and day-shift nurses, a primary care physician covering a partner’s patients, a consult team of attendings, residents, and students — and they generally speak with a unified clinical voice.
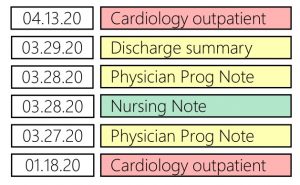
Figure 1.3. The note as thread separator. A thread is a collection of notes with similar content or purpose; under the current paradigm each note belongs to a particular thread (indicated here by color). A patient’s outpatient cardiology care is one thread; their inpatient treatment is another. Threads can overlap in time, as when inpatient care includes both physician and nursing threads.
In a note-based system, clinicians operating in different threads write different notes, some covering overlapping timeslices. This has real benefits. On the input side, multiple threads let different clinicians capture different types of information, document simultaneously in parallel, record conflicting opinions about a diagnosis or treatment, and build personalized systems for organizing information to their own needs — discipline-specific templates, dashboards, and so on. On the output side, threads provide a coarse grouping that allows basic filtration by discipline: if you want to know how the patient’s Parkinson’s disease is going, it probably makes sense to check the neurology notes.
But as with timeslices, notes are not the only way to separate information into threads — and the note-based version of threading is no match for the team-based care model now standard across the country. As the number of threads in a patient’s care grows (controlling stage II hypertension, titrating SSRIs for major depressive disorder, following weight after a new diet plan), it becomes more important that each is separated out and routed to the relevant clinicians. Yet finding the optimal grouping of clinicians into threads — who belongs together, who apart — is genuinely hard, and our choices about thread boundaries have very practical consequences. Under the current system, the same information — a physical exam, a radiology report, a lab panel — is documented many times across different clinical threads, producing duplicate data and wasted time, both in the redocumenting and in the sorting through the redundancy afterward. The more threads there are, the more time is spent documenting redundant information, the more opportunity for factual conflict and error, and the more redundant text accumulates in the chart as a whole.
2.3 The note bundles information by responsibility
Beyond organizing information by time and thread, notes serve a third major function in our healthcare system: they are groups of clinical facts that can be attested to as a single unit. By attestation, we mean a statement of agreement with, and responsibility for, a group of clinical facts. Clinically, it matters who documented what — who heard the systolic murmur, who discussed end-of-life wishes with the family, who increased the dose — to fully understand a patient’s course. We also assume medicolegal responsibility for the outcomes of our fact collection, our reasoning, and our treatment decisions. And — in some ways most importantly for the system as a whole — we state which services were performed in order to be paid.
For all these reasons, any effective documentation system must let us assign responsibility for each piece of data collected or action taken. In note-based systems, responsibility assignment happens at the note level: if Dr. X wrote a note, we assume Dr. X collected (or at least verified) everything in it. By signing the note, Dr. X attests to every fact within it in a single action.

Figure 1.4. The note as attestation bundle. When a clinician writes and signs a note, they attest to, and take responsibility for, each individual fact within it.
But writing a note is not the only way to attest to a set of clinical facts. In academic medical centers, attending physicians routinely use attestations to indicate agreement with a trainee’s or colleague’s conclusions without rewriting the same facts in their own documentation. Some EHRs let clinicians perform medication reconciliation or problem-list updates through simple attestation — a single click stating “nothing has changed” or “I agree with the current state of the chart.” This creates no new information and takes almost no time.
This, of course, is highly sensible. If only we were so sensible in every other setting of attestation. Separating the concept of attestation from the act of documentation is critical to understanding how charts become bloated with redundant, copied text. Attesting to a set of clinical facts may be necessary for billing or medicolegal purposes — but it fundamentally does not require re-documenting those facts. The two concepts have blurred together in the world of the text note. Clinicians have gotten into the habit of re-documenting old information rather than simply stating that nothing (or little) has changed. Text gets copied forward not only across timeslices within a thread, but across threads, as clinicians paste the radiology report, the consult recommendation, or another physician’s history into their own notes. One of the deepest problems with the modern note, then, is that it trains us to treat documentation and attestation as the same action. To build truly modern documentation systems, these ideas must be disentangled — not only inside EHR software, but inside our own habitual minds.
2.4 Three functions, one object
So: a note is a bundle of related clinical observations, documented at a single time, that simultaneously (1) marks off a timeslice, (2) assigns information to a clinical thread, and (3) packages facts for one-signature attestation. Any worthy documentation paradigm has to provide all three separations somehow. The question this book asks is whether one rigid object should provide all three at once — because there are many possible design decisions about how these bundlings play out, and while some yield usable systems, others yield something horribly inefficient and frustrating.
Notice what the three-function analysis already reveals. The timeslice function argues for small bundles, documented close to the moment of change. The thread function argues for bundles that persist across time. The attestation function argues for bundles shaped by billing and legal requirements, which map to neither. The note is being pulled in three directions at once, and every clinician who has stared at a blank note template wondering how much history to re-summarize has felt the tension personally.
Next, we ask where this strange three-headed object came from. The answer, in a word: paper.